Too Much Treatment
Many doctors misread lab results, according to Dan Morgan ’96, leading to unnecessary care.
When it comes to your health, have you ever worried about aegrescit medendo?
It’s not a disease; it’s a Latin phrase that means “the treatment is worse than the disease”—a potentially dangerous phenomenon.
Consider this chilling example from Dr. Dan Morgan ’96, an infectious disease and general medicine physician, who also does research as an associate professor of epidemiology and public health at the University of Maryland School of Medicine.
Writing in the Washington Post about how often physicians misread lab results, he said:
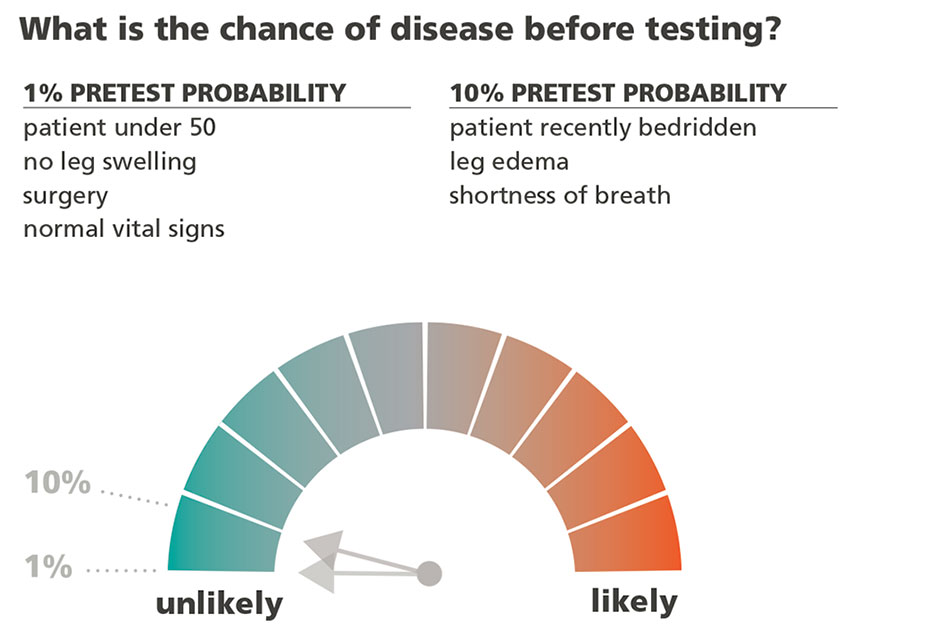
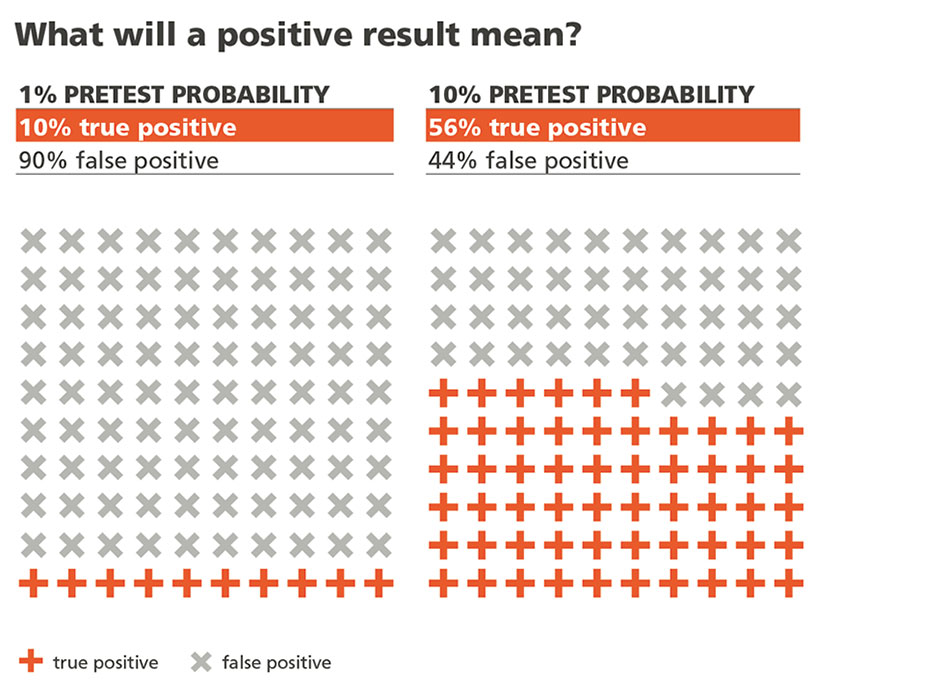
Say that Disease X has a prevalence of 1 in 1,000 (meaning that 1 out of every 1,000 people will have it), and the test to detect it has a false-positive rate of 5 percent (meaning 5 of every 100 subjects test positive for the ailment even though they don’t really have it). If a patient’s test result comes back positive, what are the chances that she actually has the disease?
In a 2014 study, researchers found that almost half of doctors surveyed said patients who tested positive had a 95 percent chance of having Disease X.
This is radically, catastrophically wrong. In fact, it’s not even close to right. Imagine 1,000 people, all with the same chance of having Disease X. We already know that just one of them has the disease. But a 5 percent false-positive rate means that 50 of the remaining 999 would test positive for it nonetheless. That means 51 people would have positive results, but only one of those would really have the illness. So if your test comes back positive, your true chance of having the disease is actually 1 out of 51, or 2 percent — a heck of a lot lower than 95 percent.
False diagnosis often leads to a cascade of unnecessary care, and is one factor driving the trend of overtreament in the U.S., estimated in a 2017 study to be more than 20%.
These are well-educated medical doctors, for heaven’s sake. What’s going on here?
“The issue is mostly that doctors, as well as patients, tend to believe that patients do or don’t have a disease when a test is positive or negative. Tests are just a lot more complicated than that,” he said.
Dan was a psych major at Reed and wrote his thesis with Prof. Dell Rhodes [1975–2006]. He remembers Reed as a place where critical thinking and taking on the status quo were encouraged. “The feeling of being a Reed College student was wanting to challenge things and wanting to question if people really knew what they were doing, or if things really worked the way we were told they worked,” he says.
For many diseases, there is only one test, so there isn’t an easy way to double-check the results. And if a test comes up positive, doctors feel the need to act.
“There’s a lot of uncertainty in medicine generally, and then having a test that people can always look back on, I think makes doctors feel more prone to do something than to not do something, even if that may not be really what’s in the patient’s best interest,” he says.
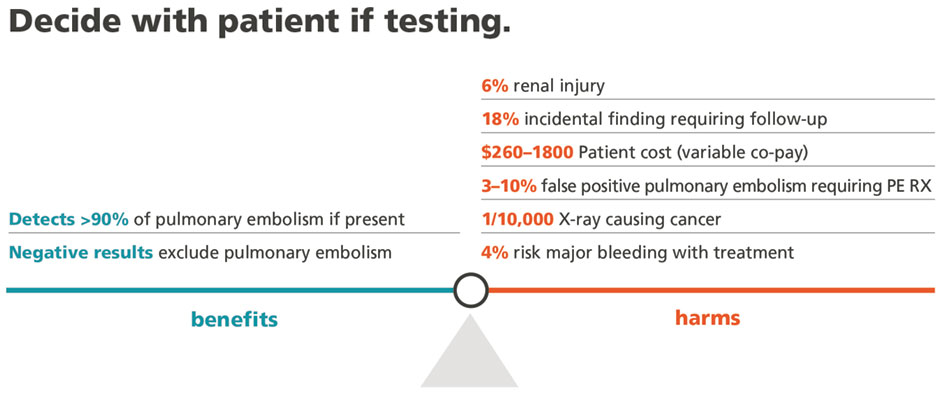
He’s working on ways to educate medical students on how to think about tests. One project involves collaborating with graphic designers to create images that clarify the probabilities. Highlighting tests that tend to have more false positives, such as mammograms, is another good way to caution physicians.
He also wants to change how doctors order tests, to make it more difficult to order the ones that are more likely to yield questionable results. The aim wouldn’t be to stop using those tests, but to nudge doctors to more fully think through the pros and cons before doing so.
The goal is to raise awareness among physicians that most tests aren’t nearly as accurate as, say, the HIV test, which is almost never wrong.
“That test is sometimes how doctors and patients think all tests work, that a test is always accurate, that a positive means you have it and a negative means you don’t,” he says. “But it’s actually the exception to the rule.”
Tags: Alumni, Health/Wellness